













Related Article
Author:- Mr. Ritesh Sharma
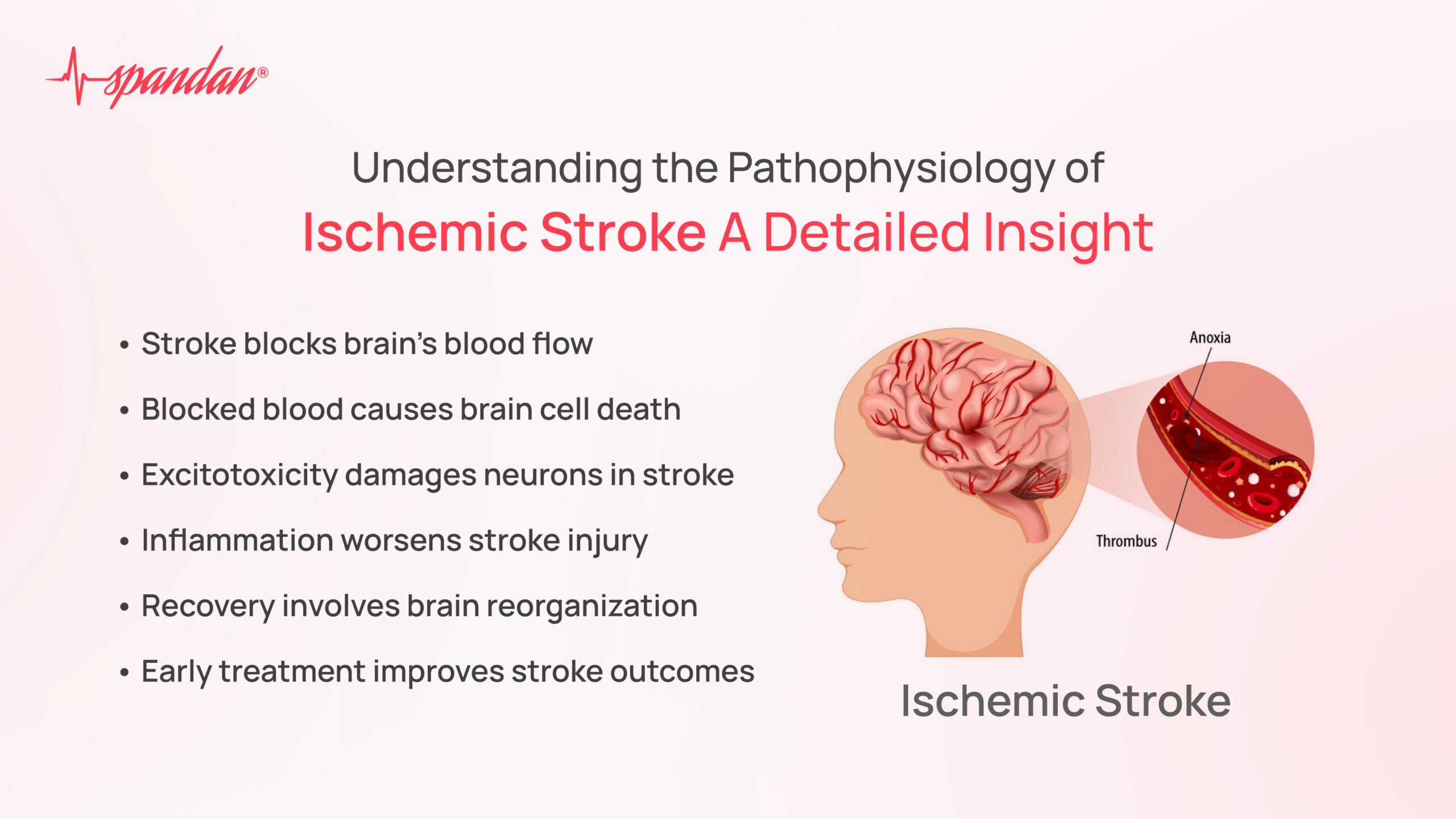
Ischemic stroke is a leading cause of disability and death worldwide, making it a crucial area of study in medical research. It occurs when the blood supply to a part of the brain is obstructed, leading to the death of brain cells. Understanding the pathophysiology of ischemic stroke is essential for the development of effective prevention and treatment strategies. In this blog, we will delve into the intricate mechanisms underlying the pathophysiology of ischemic stroke, exploring how these processes contribute to brain injury and potential therapeutic approaches.
The Basics of Ischemic Stroke
Before diving into the pathophysiology of ischemic stroke, it’s important to grasp the basic concept of this condition. An ischemic stroke occurs when a blood vessel supplying blood to the brain is blocked, typically by a blood clot or atherosclerotic plaque. This blockage prevents oxygen and nutrients from reaching brain cells, leading to cell death and subsequent neurological deficits. The severity of these deficits depends on the location and extent of the blockage.
The Pathophysiology of Ischemic Stroke
The pathophysiology of ischemic stroke is a complex process involving multiple interrelated mechanisms. These mechanisms can be broadly categorized into three stages: the initial ischemic event, the subsequent cellular responses, and the longer-term processes that contribute to brain injury.
1. The Initial Ischemic Event
The pathophysiology of ischemic stroke begins with the occlusion of a cerebral artery, most commonly due to a thrombus (a blood clot that forms in the blood vessel) or an embolus (a clot that travels from another part of the body). This occlusion leads to an immediate reduction in blood flow to the affected area of the brain, creating a region known as the ischemic core. Within this core, the lack of oxygen and glucose rapidly results in energy failure, leading to the death of neurons and other brain cells.
Surrounding the ischemic core is the penumbra, a region where blood flow is reduced but not completely cut off. In the penumbra, cells are at risk of dying but can potentially be salvaged if blood flow is restored in time. The penumbra is a critical target for therapeutic interventions aimed at reducing the overall impact of the stroke.
2. Cellular Responses to Ischemia
As ischemia sets in, the pathophysiology of ischemic stroke progresses through a series of cellular responses that exacerbate brain injury. One of the earliest responses is the depletion of adenosine triphosphate (ATP), the energy currency of the cell. Without sufficient ATP, the sodium-potassium pumps in cell membranes fail, leading to an influx of sodium and calcium ions into neurons.
This ionic imbalance triggers a cascade of damaging events, including the release of glutamate, an excitatory neurotransmitter. Excessive glutamate in the synaptic cleft overstimulates its receptors, particularly NMDA (N-methyl-D-aspartate) receptors, leading to further calcium influx. This phenomenon, known as excitotoxicity, is a key component of the pathophysiology of ischemic stroke. Excessive calcium within neurons activates various enzymes that degrade cellular components, contributing to cell death.
Another critical aspect of the pathophysiology of ischemic stroke is the formation of free radicals. Ischemia and the subsequent reperfusion (restoration of blood flow) generate reactive oxygen species (ROS) and reactive nitrogen species (RNS), which can damage cellular membranes, proteins, and DNA. This oxidative stress further exacerbates neuronal injury and promotes inflammation.
3. Inflammatory Response and Blood-Brain Barrier Breakdown
Inflammation plays a central role in the pathophysiology of ischemic stroke. Shortly after the onset of ischemia, immune cells, including microglia (the brain’s resident immune cells) and peripheral immune cells, are activated and migrate to the site of injury. These cells release pro-inflammatory cytokines, chemokines, and other mediators that exacerbate neuronal damage.
The inflammatory response also contributes to the breakdown of the blood-brain barrier (BBB), a protective barrier that normally prevents harmful substances from entering the brain. When the BBB is compromised, harmful substances such as immune cells, proteins, and fluid can infiltrate the brain tissue, leading to cerebral edema (swelling of the brain) and increased intracranial pressure. This further contributes to the pathophysiology of ischemic stroke by worsening brain injury.
Long-Term Consequences of Ischemic Stroke
The pathophysiology of ischemic stroke is not limited to the acute phase but extends into the subacute and chronic phases. In the days and weeks following the initial stroke, secondary processes such as apoptosis (programmed cell death), neuroinflammation, and neurodegeneration continue to shape the outcome of the stroke.
Apoptosis is a significant contributor to delayed neuronal death in the penumbra and other brain regions affected by ischemia. This process is regulated by various molecular pathways, including the activation of caspases, a family of proteases that execute the apoptotic program. Targeting apoptosis is a potential therapeutic strategy in the context of ischemic stroke.
Neuroinflammation, driven by persistent activation of microglia and astrocytes, also plays a crucial role in the long-term pathophysiology of ischemic stroke. While inflammation is necessary for clearing dead cells and promoting tissue repair, excessive or prolonged inflammation can lead to further damage and impede recovery. Modulating the inflammatory response is another potential avenue for stroke treatment.
Finally, the pathophysiology of ischemic stroke includes neuroplasticity and brain repair mechanisms. Neuroplasticity refers to the brain’s ability to reorganize and form new neural connections in response to injury. In the context of stroke, neuroplasticity underlies the recovery of lost functions through the reorganization of surviving brain networks. Rehabilitation strategies that promote neuroplasticity, such as physical therapy and cognitive training, are essential for improving outcomes in stroke survivors.
Therapeutic Implications
Understanding the pathophysiology of ischemic stroke has important implications for developing effective treatments. Currently, the most effective treatment for ischemic stroke is reperfusion therapy, which involves the use of thrombolytic agents (e.g., tissue plasminogen activator, or tPA) or mechanical thrombectomy to restore blood flow to the affected brain region. However, these treatments are time-sensitive and must be administered within a narrow therapeutic window to be effective.
Beyond reperfusion, research into neuroprotective agents aims to target various aspects of the pathophysiology of ischemic stroke, such as excitotoxicity, oxidative stress, inflammation, and apoptosis. While many neuroprotective agents have shown promise in preclinical studies, translating these findings into effective clinical treatments has been challenging. The complexity of stroke pathophysiology and the variability in individual responses to treatment contribute to these challenges.
The pathophysiology of ischemic stroke is a multifaceted process involving an interplay of cellular, molecular, and systemic mechanisms that contribute to brain injury and recovery. By unraveling these complex processes, researchers and clinicians can develop more targeted and effective therapies to improve outcomes for stroke patients. Continued research into the pathophysiology of ischemic stroke holds the promise of reducing the burden of this devastating condition and enhancing the quality of life for stroke survivors.